Target Trial Emulation in Pregnancy Research
2024-10-31
Introduction
Today’s goals
- Understand the target trial framework and why it’s useful in reproductive and perinatal research
- Explore different types of pregnancy research questions that may be addressed with this approach
- Discover some intuition behind the clone-censor-weighting approach through a numeric example
Why pregnancy research is challenging
- Complex timing issues (exposure, outcomes, competing events)
- Immortal time bias is pervasive
- Multiple individuals (pregnant person, fetus, child)
- Need for clarity about what we’re estimating
One solution
The target trial framework forces us to be explicit about who, what, when, and how (I guess where too, but not usually as much of a problem!)
One problem: time zero
Many observational studies don’t have a clear “time zero” when treatment assignment occurs
Example: Comparing pregnancy outcomes in:
- People who took antidepressants during pregnancy
- People who didn’t take antidepressants during pregnancy
When are they “assigned” to exposure groups?
Immortal time bias
If we define groups based on what actually happened during pregnancy:
- “Exposed” group = those who took medication at some point
- “Unexposed” group = those who never took medication
The exposed group had to survive long enough (e.g. remain pregnant) to take the medication!
- This is a problem whenever the outcome depends on time (i.e., not just survival)
What is a target trial?
A hypothetical randomized trial that would answer your causal question if it could be conducted
Note
The target trial is a design concept, not an analysis method. It has guided study design in epidemiology for decades but recently popularized as an explicit framework (Hernán and Robins 2016).
Why a trial?
Randomized trials have clear advantages for causal inference:
- Randomization at baseline
- Not the case in observational data no matter what we do, but we can try with good confounder measurement and reasonable eligibility criteria
- Stringent eligibility criteria
- Everyone who enters the study has equipoise for the treatment strategies being compared
Why a trial?
Randomized trials have clear advantages for causal inference:
- Clear time zero
- Everyone is assigned to treatment and starts follow-up at the same time
- We can make this happen in observational data with careful design
- Well-defined treatment strategies
- In order to give participants their assigned treatment, people have to have rules to follow!
- We can define these rules in observational data too
Why a target trial?
We know we can’t run the randomized trial we want to conduct to answer our causal question (lack of resources, unethical to randomize, impossible to provide certain treatments/exposures, too many years of follow-up needed, too many treatment strategies to compare, etc.)
- But we can design it hypothetically
- And then try to emulate it as closely as possible with observational data
Emulating a target trial
The observational study should be designed so as to match up with this trial as closely as possible
Warning
Don’t jump straight to emulation without carefully thinking through the trial, though it can be helpful to think ahead. Compromises in emulation should be explicit and justified.
Essential components
- Eligibility criteria
- Treatment strategies
- Assignment procedures
- Follow-up period
- Outcome(s)
- Causal contrast(s)
- Statistical analysis plan
Note
Recently published guidelines for reporting target trial emulations detail these components: Cashin et al. (2025)
Eligibility criteria: the “who”
Besides making for a clearer question with more practical implications, eligibility criteria can help address confounding in the emulation by ensuring everyone included has a reasonable chance of getting the treatment strategies being compared*
- We might exclude people with contraindications to treatment, or those who would never consider it
- This often means defining pregnancy status and gestational age at time zero carefully
Time zero: the “when”
The eligibility criteria also define when people enter the study
- Time zero occurs when people meet eligibility criteria (and in a trial, agree to be randomized)
- We could imagine scenarios where people meet eligibility repeatedly over time (e.g., at every antenatal care visit)
- We can take this into account when emulating
Treatment strategies: the “what” and “how”
Each strategy represents an intervention we could imagine putting in motion at time zero for a given treatment arm:
- Immediately upon randomization, tell everyone to get treatment (e.g., a vaccination)
- At 6 weeks gestation (time zero), tell everyone to start treatment at 12 weeks gestation but not before
- Tell everyone to wait until 20 weeks to start treatment
- Tell everyone to start treatment when symptoms appear
This is easier for some causal questions than others
- Pharmaceutical interventions with fixed timing (e.g., vaccination at week 32 vs. no vaccination)
- Procedure at some known clinical event (e.g., cerclage at diagnosis of short cervix vs. no cerclage)
- Comparisons of two treatments with the same indication
Tip
It’s helpful to read through existing randomized trials on similar questions to see how they defined these components, see clinicaltrials.gov for ideas!
Pharmaceutical example (Zidan et al. (2025))
| Components | Target trial |
|---|---|
| Causal question | What is the effect of SARS-CoV-2 mRNA vaccine BNT162b2 on COVID-19? |
| Eligibility criteria | Inclusion criteria:
Exclusion criteria:
|
| Treatment strategies | 1. Two vaccination doses 2. No SARS-CoV-2 vaccination until the end of pregnancy |
| Assignment procedures | 1:1 randomization into the two treatment arms, stratified by gestational week |
| Follow-up | Since administering the first dose and up to 1 month post delivery |
| Outcome | SARS-CoV-2 infection as determined by positive PCR test or clinical COVID-19 diagnosis |
| Causal contrast | Incidence rate ratios; intention-to-treat (one vaccine dose) and per-protocol (two doses) |
Other types of questions
It may feel weird to design a target trial for other types of causal questions
- Unethical/impossible to randomize
- e.g., harmful exposures, social determinants of health
It’s worth thinking through anyway to make sure you are clear about your causal question of interest (you don’t have to publish it as a “target trial”!)
Non-pharmaceutical example (Smith et al. (2022))
| Components | Target trial | |
| Causal question | What is the effect of COVID-19 infection on preterm delivery? | |
| Eligibility criteria | 1. Pregnant individuals with gestational age 12-36 weeks. 2. No known previous SARS-CoV-2 infection 3. No previous vaccination for COVID-19 |
|
| Treatment strategies | 1. Symptomatic COVID-19 within a week after enrollment. 2. No SARS-CoV-2 infection for the rest of the pregnancy. |
|
| Assignment procedures | Randomization at enrollment, stratified by gestational age (in weeks). | |
| Follow-up | Patients are followed from the time of COVID-19 testing or enrollment (time zero) until delivery, loss to follow-up, or administrative end of follow-up. | |
| Outcome | Preterm delivery, defined as delivery before 37 completed weeks of gestation. | |
| Causal contrast | Intention-to-treat effect on the risk ratio and risk difference scales for each gestational week (time zero) |
Notes on these components and things to think about in emulation (hopefully not compromises to the integrity of the target trial)
| Components | Target trial | |
| Eligibility criteria |
|
|
| Treatment strategies |
|
|
| Assignment procedures |
|
|
| Follow-up |
|
|
| Outcome |
|
|
| Causal contrast |
|
Examples
Avalos et al. (2023)
Caniglia et al. (2018)
Chiu et al. (2024)
Wong et al. (2024)
Discussion
- What was the causal question?
- What were the key components of the target trial protocol, including eligibility criteria, treatment strategies, etc. What was time zero?
- What made this question challenging to design an “emulatable” target trial?
- How did the authors handle the challenge? Were there compromises made?
Avalos et al. (2023) - Treating hypertension at different thresholds
Key features/challenges:
- Treatment strategies are dynamic - depend on clinical measurements, don’t know ahead of time who will need treatment when
- People can be part of multiple treatment groups over time
Caniglia et al. (2018) - Antiretroviral therapy started before conception
Key features/challenges:
- Treatment/time zero occurs before pregnancy
- Competing event: not getting pregnant
- Can’t condition on pregnancy without bias
- Treatment strategy includes getting pregnant within a certain time frame
Chiu et al. (2024) - Metformin in first trimester
Key features/challenges:
- Treatment happens early in pregnancy
- Competing risks: pregnancy loss – can’t observe malformations without live birth
- Use of composite outcome
Wong et al. (2024) - COVID-19 antiviral within 5 days of infection
Key features/challenges:
- Treatment must start within a short window after infection (grace period)
- Rare exposure, rare outcomes
Common themes across papers
- Time zero must be clearly defined
- Before hypertension (Avalos)
- Preconception (Caniglia)
- Early pregnancy (Chiu)
- At sympomatic infection (Wong)
- Strategies must be realistic and well-defined
- Not just “exposed vs. unexposed”
- Include rules for what happens over time, e.g., grace period, blood pressure monitoring
- Competing events are common in pregnancy
- Not conceiving competes with pregnancy outcomes
- Pregnancy loss competes with later outcomes
Thoughts/questions
Emulating target trials with clone-censor weighting
This example is somewhat based on an example about comparing duration of treatment in Hernán (2018)
Does vaccination timing in pregnancy affect live birth?
Eligibility: Unvaccinated, at/soon after conception
Treatment strategies:
- Strategy 0: Never vaccinate during pregnancy
- Strategy 1: Vaccinate in trimester 1 only
- Strategy 2: Vaccinate in trimester 2 only
- Strategy 3: Vaccinate in trimester 3 only
Outcome: Live birth (yes/no)
Pregnancy timeline
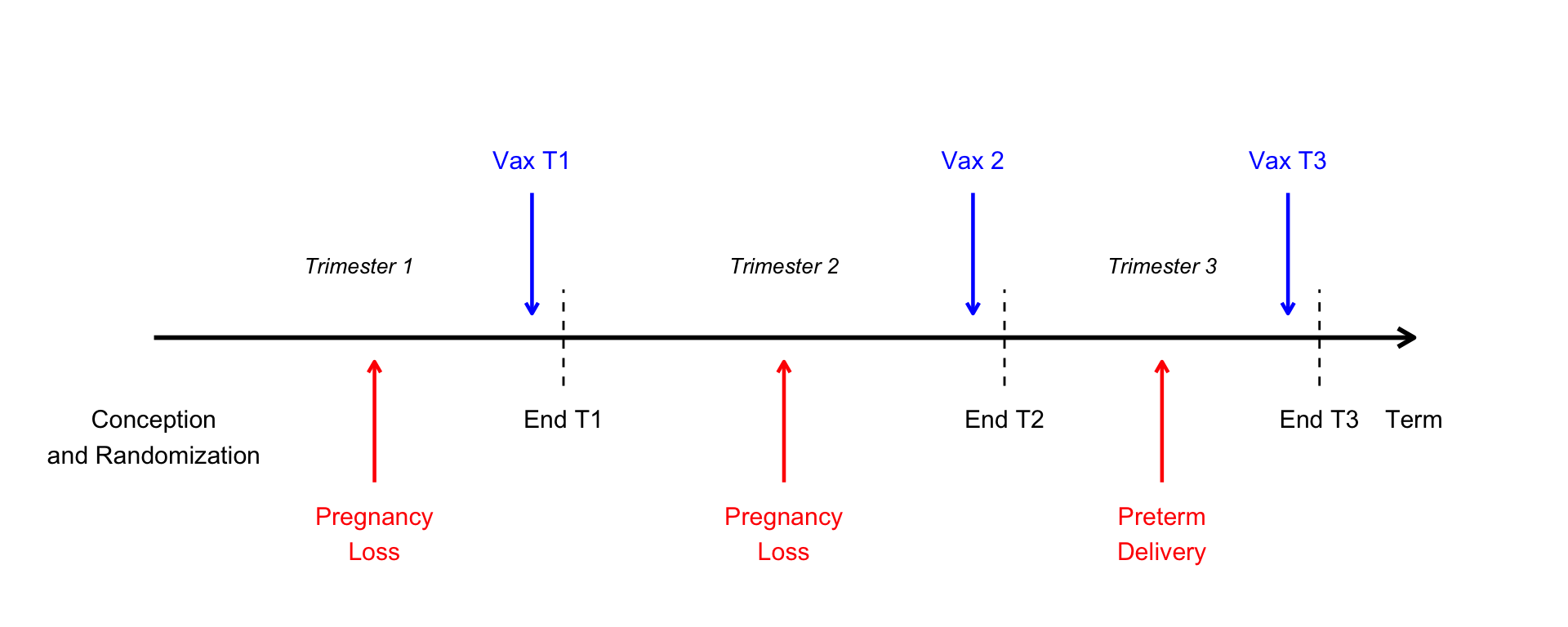
Note
We are simplifying things by assuming vaccination happens at the end of a trimester, after any pregnancy losses
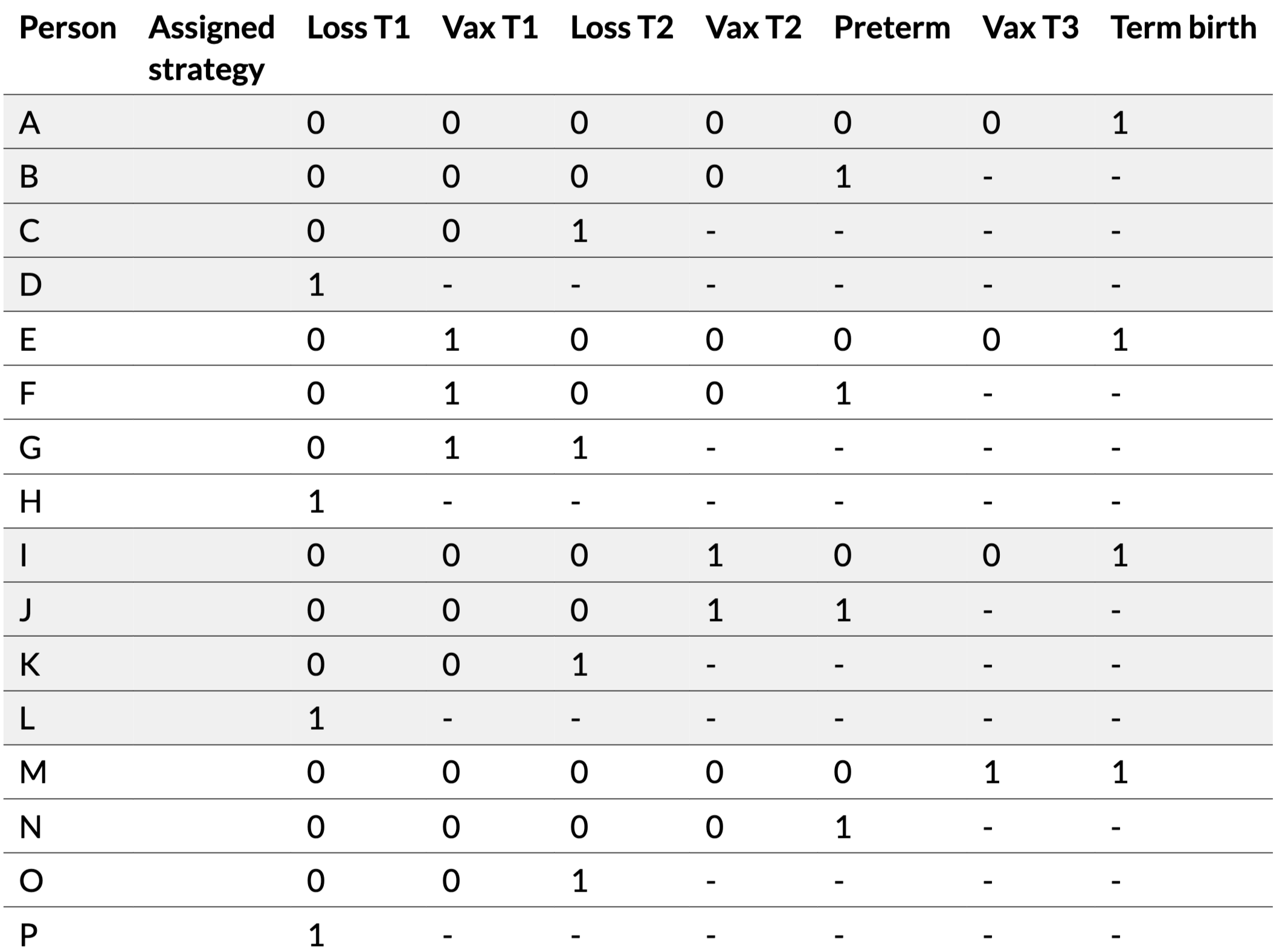
Randomized trial data
16 pregnant people randomly assigned to 4 strategies:
| Person | Assigned strategy | Loss T1 | Vax T1 | Loss T2 | Vax T2 | Preterm | Vax T3 | Term birth | Live birth |
|---|---|---|---|---|---|---|---|---|---|
| A | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 |
| B | 0 | 0 | 0 | 0 | 0 | 1 | - | - | 1 |
| C | 0 | 0 | 0 | 1 | - | - | - | - | 0 |
| D | 0 | 1 | - | - | - | - | - | - | 0 |
| E | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 |
| F | 1 | 0 | 1 | 0 | 0 | 1 | - | - | 1 |
| G | 1 | 0 | 1 | 1 | - | - | - | - | 0 |
| H | 1 | 1 | - | - | - | - | - | - | 0 |
| I | 2 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 |
| J | 2 | 0 | 0 | 0 | 1 | 1 | - | - | 1 |
| K | 2 | 0 | 0 | 1 | - | - | - | - | 0 |
| L | 2 | 1 | - | - | - | - | - | - | 0 |
| M | 3 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 |
| N | 3 | 0 | 0 | 0 | 0 | 1 | - | - | 1 |
| O | 3 | 0 | 0 | 1 | - | - | - | - | 0 |
| P | 3 | 1 | - | - | - | - | - | - | 0 |
Randomized trial results
By assigned strategy:
| Assigned strategy | N | Live births | Probability |
|---|---|---|---|
| 0 | 4 | 2 | 0.5 |
| 1 | 4 | 2 | 0.5 |
| 2 | 4 | 2 | 0.5 |
| 3 | 4 | 2 | 0.5 |
All strategies have 50% live birth rate (we are operating in a situation where the null hypothesis of no effect of vaccination at any time is true)
Moving to observational data
In observational data, we don’t see the assigned strategy.
We only see what actually happened:
- When (if) people got vaccinated
- When pregnancy losses occurred
- Whether there was a live birth and when
Let’s classify people by observed vaccination status and timing…
Observed data
Same 16 people, but now we don’t know their assigned strategy:
| Person | Observed treatment | Loss T1 | Vax T1 | Loss T2 | Vax T2 | Preterm | Vax T3 | Term birth | Live birth |
|---|---|---|---|---|---|---|---|---|---|
| A | 0 (Never) | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 |
| B | 0 (Never) | 0 | 0 | 0 | 0 | 1 | - | - | 1 |
| C | 0 (Never) | 0 | 0 | 1 | - | - | - | - | 0 |
| D | 0 (Never) | 1 | - | - | - | - | - | - | 0 |
| E | 1 (Vax T1) | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 |
| F | 1 (Vax T1) | 0 | 1 | 0 | 0 | 1 | - | - | 1 |
| G | 1 (Vax T1) | 0 | 1 | 1 | - | - | - | - | 0 |
| H | 0 (Never) | 1 | - | - | - | - | - | - | 0 |
| I | 2 (Vax T2) | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 |
| J | 2 (Vax T2) | 0 | 0 | 0 | 1 | 1 | - | - | 1 |
| K | 0 (Never) | 0 | 0 | 1 | - | - | - | - | 0 |
| L | 0 (Never) | 1 | - | - | - | - | - | - | 0 |
| M | 3 (Vax T3) | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 |
| N | 0 (Never) | 0 | 0 | 0 | 0 | 1 | - | - | 1 |
| O | 0 (Never) | 0 | 0 | 1 | - | - | - | - | 0 |
| P | 0 (Never) | 1 | - | - | - | - | - | - | 0 |
Naive analysis: by achieved vaccination
Classify by when they actually got vaccinated:
| Observed vaccination | N | Live births | Probability |
|---|---|---|---|
| 0 (Never) | 10 | 3 | 0.30 |
| 1 (Vax T1) | 3 | 2 | 0.67 |
| 2 (Vax T2) | 2 | 2 | 1.00 |
| 3 (Vax T3) | 1 | 1 | 1.00 |
The problem: immortal time bias!
Later vaccination appears highly protective!
But: People who got vaccinated later had to survive to that point
- All of the pregnancy losses get assigned to the “Never” or “Vax T1” groups
- By the time people are classified as “Vax T2” or “Vax T3”, they have already survived those earlier periods
Think like a randomized trial
In a randomized trial, people are assigned to strategies at time zero – even if they don’t get treatment (by choice, not surviving long enough, etc.), they are analyzed in their assigned group*
Immortal time bias
Generally the not-treated group will underestimate the true risk, and the treated group will overestimate it (the later treated, or longer duration required, the more the bias):
| Strategy | True probability | Naive estimate | Bias |
|---|---|---|---|
| 0 (Never) | 0.50 | 0.30 | ↓ |
| 1 (Vax T1) | 0.50 | 0.67 | ↑ |
| 2 (Vax T2) | 0.50 | 1.00 | ↑↑ |
| 3 (Vax T3) | 0.50 | 1.00 | ↑↑ |
This makes treatment appear to reduce risk when there is actually no effect (or if there were a true effect of treatment, this might mask it)
Emulation via clone-censor-weighting
Pretend you have a randomized trial in which everyone is assigned to all strategies at time zero:
- Clone everyone to all compatible strategies
- Censor clones when they deviate from assigned strategy
- Weight to correct for selection bias from censoring
Step 1: Cloning
For each person, create clones for all treatment strategies
| Person | Assigned strategy | Loss T1 | Vax T1 | Loss T2 | Vax T2 | Preterm | Vax T3 | Term birth | Live birth |
|---|---|---|---|---|---|---|---|---|---|
| A-0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 |
| B-0 | 0 | 0 | 0 | 0 | 0 | 1 | - | - | 1 |
| C-0 | 0 | 0 | 0 | 1 | - | - | - | - | 0 |
| D-0 | 0 | 1 | - | - | - | - | - | - | 0 |
| E-0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 |
| F-0 | 0 | 0 | 1 | 0 | 0 | 1 | - | - | 1 |
| G-0 | 0 | 0 | 1 | 1 | - | - | - | - | 0 |
| H-0 | 0 | 1 | - | - | - | - | - | - | 0 |
| I-0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 |
| J-0 | 0 | 0 | 0 | 0 | 1 | 1 | - | - | 1 |
| K-0 | 0 | 0 | 0 | 1 | - | - | - | - | 0 |
| L-0 | 0 | 1 | - | - | - | - | - | - | 0 |
| M-0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 |
| N-0 | 0 | 0 | 0 | 0 | 0 | 1 | - | - | 1 |
| O-0 | 0 | 0 | 0 | 1 | - | - | - | - | 0 |
| P-0 | 0 | 1 | - | - | - | - | - | - | 0 |
Treatment strategy Vax T1
| Person | Assigned strategy | Loss T1 | Vax T1 | Loss T2 | Vax T2 | Preterm | Vax T3 | Term birth | Live birth |
|---|---|---|---|---|---|---|---|---|---|
| A-1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 |
| B-1 | 1 | 0 | 0 | 0 | 0 | 1 | - | - | 1 |
| C-1 | 1 | 0 | 0 | 1 | - | - | - | - | 0 |
| D-1 | 1 | 1 | - | - | - | - | - | - | 0 |
| E-1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 |
| F-1 | 1 | 0 | 1 | 0 | 0 | 1 | - | - | 1 |
| G-1 | 1 | 0 | 1 | 1 | - | - | - | - | 0 |
| H-1 | 1 | 1 | - | - | - | - | - | - | 0 |
| I-1 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 |
| J-1 | 1 | 0 | 0 | 0 | 1 | 1 | - | - | 1 |
| K-1 | 1 | 0 | 0 | 1 | - | - | - | - | 0 |
| L-1 | 1 | 1 | - | - | - | - | - | - | 0 |
| M-1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 |
| N-1 | 1 | 0 | 0 | 0 | 0 | 1 | - | - | 1 |
| O-1 | 1 | 0 | 0 | 1 | - | - | - | - | 0 |
| P-1 | 1 | 1 | - | - | - | - | - | - | 0 |
And so on…
Step 2: Censoring
Censor clones when their observed data becomes incompatible with assigned strategy:
- Strategy 0 (never): censor if vaccinated in T1, T2, or T3
- Strategy 1 (vax T1): censor if not vaccinated in T1
- Strategy 2 (vax T2): censor if vaccinated in T1 or not vaccinated in T2
- Strategy 3 (vax T3): censor if vaccinated in T1 or T2 or not vaccinated in T3
If there is a pregnancy loss in T1, do not censor afterward–we don’t know whether they would have gotten vaccinated or not (can contribute to multiple strategies)
Censoring
- This is why defining the treatment strategies precisely is incredibly important, more so than in a real trial
- In real life, “clinical judgment” may result in someone stopping treatment
- In your emulation, should you censor someone if they stop treatment? Or would they be “allowed” to stop in a real trial?
- If everyone ends up censored, you’re trying to study a treatment strategy for which you have no positivity!
- Come up with a new strategy that allows more flexibility!
Practice censoring
Step 3: Weighting
Selection bias introduced by censoring must be corrected
Use inverse probability weighting:
- Weight = 1 / (probability of remaining uncensored)
- This would be conditional on current values of covariates if we had them
- Transfers weight from censored to uncensored observations
Calculating probability of remaining uncensored
This varies over time, and can be calculated as the product of interval-specific probabilities:
\[ \text{Prob(uncensored at time } t) = \prod_{k=0}^{t} \text{Prob(uncensored at } k \mid \text{uncensored at } k-1) \]
That is, the probability of still being uncensored at the end of T3 is:
the probability of not being censored in T1
times the probability of not being censored in T2 (given not censored in T1)
times the probability of not being censored in T3 (given not censored in T1 or T2)
Original Data
# A tibble: 16 × 10
person assigned loss_t1 vax_t1 loss_t2 vax_t2 preterm vax_t3 term livebirth
<chr> <dbl> <dbl> <dbl> <dbl> <dbl> <dbl> <dbl> <dbl> <dbl>
1 A 0 0 0 0 0 0 0 1 1
2 B 0 0 0 0 0 1 NA NA 1
3 C 0 0 0 1 NA NA NA NA 0
4 D 0 1 NA NA NA NA NA NA 0
5 E 1 0 1 0 0 0 0 1 1
6 F 1 0 1 0 0 1 NA NA 1
7 G 1 0 1 1 NA NA NA NA 0
8 H 1 1 NA NA NA NA NA NA 0
9 I 2 0 0 0 1 0 0 1 1
10 J 2 0 0 0 1 1 NA NA 1
11 K 2 0 0 1 NA NA NA NA 0
12 L 2 1 NA NA NA NA NA NA 0
13 M 3 0 0 0 0 0 1 1 1
14 N 3 0 0 0 0 1 NA NA 1
15 O 3 0 0 1 NA NA NA NA 0
16 P 3 1 NA NA NA NA NA NA 0Step 1: Cloning
Each person is cloned into 4 copies (one for each vaccination strategy: 0, 1, 2, 3)
# A tibble: 4 × 2
strategy n
<int> <int>
1 0 16
2 1 16
3 2 16
4 3 1616 people × 4 strategies = 64 rows
Step 2: Censoring
censored_data <- cloned_data %>%
mutate(
# T1: only at risk if survived T1
censored_t1 = case_when(
loss_t1 == 1 ~ NA, # Already had outcome
strategy %in% c(0, 2, 3) & vax_t1 == 1 ~ TRUE, # Deviated by vaccinating
strategy == 1 & vax_t1 == 0 ~ TRUE, # Deviated by not vaccinating
.default = FALSE # Followed strategy
),
# T2: only at risk if uncensored and unvaccinated at T1 and survived T2
censored_t2 = case_when(
is.na(censored_t1) | censored_t1 ~ NA, # Already censored or had outcome at T1
loss_t2 == 1 ~ NA, # Had outcome at T2
vax_t1 == 1 ~ NA, # Already had vax at T1
strategy %in% c(0, 3) & vax_t2 == 1 ~ TRUE, # Deviated by vaccinating
strategy == 2 & vax_t2 == 0 ~ TRUE, # Deviated by not vaccinating
.default = FALSE # Followed strategy
),
# T3: only at risk if uncensored and unvaccinated at T2 and survived T3
censored_t3 = case_when(
is.na(censored_t2) | censored_t2 ~ NA, # Already censored or had outcome at T2
preterm == 1 ~ NA, # Had outcome at T3
vax_t1 == 1 | vax_t2 == 1 ~ NA, # Already had vax at T1 or T2
strategy == 0 & vax_t3 == 1 ~ TRUE, # Deviated by vaccinating
strategy == 3 & vax_t3 == 0 ~ TRUE, # Deviated by not vaccinating
.default = FALSE # Followed strategy
),
# Final censoring: censored if ANY time point is TRUE
censored = (censored_t1) | (censored_t2) | (censored_t3),
censored = replace_na(censored, FALSE)
)Censoring Summary
Different numbers contribute to each strategy:
# A tibble: 4 × 7
strategy n_total censored_t1 censored_t2 censored_t3 total_censored uncensored
<int> <int> <int> <int> <int> <int> <int>
1 0 16 3 2 1 6 10
2 1 16 9 0 0 9 7
3 2 16 3 4 0 7 9
4 3 16 3 2 1 6 10Step 3a: Calculate Censoring Probabilities
Probability of vaccination can be used to calculate interval-specific censoring probabilities
- Set up the data so that people who aren’t eligible to be censored at a given timepoint don’t contribute (have
NAfor vaccination status and/or subset to those not previously censored or vaccinated - Model the probability of treatment (i.e., a propensity score model!)
Vaccination in T1 = censoring (strategy 0, 2, and 3) or not (strategy 1)
A B C E F G I J K M N O
0 0 0 1 1 1 0 0 0 0 0 0 1
0.25 Vaccination in T2 = censoring (strategy 0 and 3) or not (2)
(For strategy 1, already censored if not vaccinated in T1 so no one “at risk for” censoring here)
Vaccination in T3 = censoring (strategy 0) or not (3)
(For strategies 1 and 2, already censored if not vaccinated in T1 or T2 so no one “at risk for” censoring here)
Step 3b: Calculate Weights
Weight = 1 / (cumulative probability of not being censored)
weighted_data <- censored_data %>%
mutate(
# Probability of not being censored at each time point
prob_not_cens_t1 = case_when(
is.na(censored_t1) ~ 1, # Not at risk
strategy == 1 ~ p_vax_t1, # Strategy 1: needs vax at T1
strategy %in% c(0, 2, 3) ~ 1 - p_vax_t1, # No vax at T1
TRUE ~ 1
),
prob_not_cens_t2 = case_when(
is.na(censored_t2) ~ 1, # Not at risk
strategy == 2 ~ p_vax_t2, # Strategy 2: needs vax at T2
strategy %in% c(0, 3) ~ 1 - p_vax_t2, # No vax at T2
TRUE ~ 1
),
prob_not_cens_t3 = case_when(
is.na(censored_t3) ~ 1, # Not at risk
strategy == 3 ~ p_vax_t3, # Strategy 3: needs vax at T3
strategy == 0 ~ 1 - p_vax_t3, # No vax at T3
TRUE ~ 1
),
# Cumulative probability = product
cum_prob_not_censored = prob_not_cens_t1 * prob_not_cens_t2 * prob_not_cens_t3,
# Weight = inverse probability (only for uncensored)
weight = if_else(!censored, 1 / cum_prob_not_censored, 0)
)Example: Strategy 0 (Never vaccinate)
Uncensored individuals and their weights:
Step 3c: Calculate Weighted Outcomes
# A tibble: 4 × 4
strategy sum_weights weighted_livebirths risk_livebirth
<int> <dbl> <dbl> <dbl>
1 0 16.0 8.00 0.500
2 1 16.0 8.00 0.500
3 2 16.0 8.00 0.500
4 3 16.0 8.00 0.500Why it works
The three steps:
- Cloning eliminates immortal time bias by assigning strategies at time zero
- Censoring ensures clones follow their assigned strategy
- Weighting corrects for selection bias introduced by censoring
Key assumptions
- No unmeasured confounding (of baseline treatment and treatment continuation/discontinuation, i.e., time-varying confounding)
- Correct specification of censoring models
- There are many different modeling assumptions we could make, e.g., one model for vaccination with a term for time, or separate models at each time point
- Positivity (some probability of continuing the treatment strategy at each time)
When to use clone-censor-weighting
- Treatment duration comparisons
- Sustained treatment strategies that evolve over time
- Variable timing of exposure
- Threshold-based or dynamic treatment rules
- Any strategy where assignment isn’t identifiable at time zero
- Multiple cycles or sequential treatment decisions
Practical considerations
- Descriptive analysis of treatment patterns
- Check positivity (can strategies actually be followed?)
- How will you define confounders (both baseline and time-varying)
- Start with simple examples to develop code
- Check weight distributions
Extensions and advanced topics
- Grace periods for treatment initiation
- Nested sequential trials
- Joint strategies (treatment + monitoring)
Helpful/interesting papers
Hernán et al. (2008) Cain et al. (2010) Young et al. (2011) Hernán et al. (2016) Hernán and Robins (2016) Labrecque and Swanson (2017) Hernán (2018) Caniglia et al. (2019) Dickerman et al. (2019) Chiu et al. (2020) Maringe et al. (2020) Ben-Michael et al. (2021) Gaber et al. (2024) Cashin et al. (2025) Fu et al. (2026) Moreno-Betancur et al. (2025)
Discussion/Questions
What pregnancy research questions are you working on?
How might you apply target trial thinking?
What challenges do you anticipate?
What tools or resources would be most helpful?
Thank you!
email: l.smith@northeastern.edu